What is an Acoustic Neuroma / Schwannoma?
DR PREM PILLAY,
SENIOR CONSULTANT NEUROSURGEON,
ACOUSTIC NEUROMA AND SCHWANNOMA EXPERT
(Higher Training in Brain Tumors -Residency and Chief Resident, the Cleveland Clinic Foundation Hospital, Fellow in Neurosurgical Oncology at MD Anderson Cancer Center and Hospital, USA)
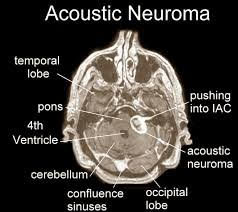

Definition: An acoustic neuroma is an intra-cranial (within the head but outside the brain) tumor that arises from the superior vestibular nerve (a nerve for balance). The more accurate term is therefore vestibular schwannoma.
Histopathology: They are firm and encapsulated and classified as benign. Antoni A and Antoni B biphasic patterns are found. They can be cystic, hemorrhagic or entirely solid tumors. Malignancy is rare.
Location: It starts in the internal acoustic meatus but can grow medially towards the brainstem and occupy space in the cerebellopontine angle.
Related tumors: Trigeminal schwannoma, facial nerve schwannoma, hypoglossal schwannoma and glossopharyngeal nerve schwannoma, can occur in the same location (Cerebellar Pontine Angle or CP angle).
Symptoms / Presentation: This includes tinnitus (ringing in the ears), hearing loss, imbalance, numbness of the face, weakness of the face, difficulty in chewing and swallowing (caused by compressing nerves, brainstem and cerebellum in the CP angle as the tumor grows). Large tumors may cause hydrocephalus by obstructing CSF circulation and this may cause symptoms related to this condition. Large tumors may cause coma, paralysis and death.
Diagnosis: It can be overlooked in the early stages and the diagnosis missed as tinnitus and mild hearing loss are often not investigated with MRI scanning. The best single test is MRI of the brain and IAM (internal acoustic meatus) with contrast (gadolinium). Hearing and balance tests can document the effects of the tumor.
Treatment:
There are in general, three options: Monitoring of small tumors (< 1cm in size) if hearing is still intact is an option in older patients and in younger patients with bilateral tumors associated with NF (Neurofibromatosis, NF-2). This includes clinical and hearing tests supplemented with regular MRI scans. If the tumor increases in size and significant hearing loss occurs treatment is recommended.
Surgery and tumor excision was once the only treatment option for most of the 20th century. Microsurgery, improved anesthesiology, Image-guidance , better microsurgical tools and nerve monitoring have improved the results of surgery. Microsurgery may still be the best treatment option for large tumors (>3.5cm) in selected patients who have symptoms from the mass effect of the tumor.
Radiosurgery is now an accepted treatment modality for acoustic neuromas as there is overall a lower risk than surgery in terms of anesthesia risks, bleeding and infection. Mortality which is a possibility with any brain surgery is extremely rare and even exceptional with modern radiosurgery/stereotactic radiotherapy. In addition numerous centers and clinical papers have documented the safety and effectiveness of Radiosurgery. Newer forms of radiosurgery include Micro-MLC radiosurgery, fractionated radiosurgery (also referred to as Stereotactic Radiotherapy and vice versa) and Proton beam therapy.
Combined Microsurgery and Radiosurgery (CMR) is an option that can work well with large acoustic neuromas and schwannomas of the CP angle. Microsurgery is used to remove tumor in a safe way without damaging near by nerves (especially the facial nerve and trigeminal nerve and the brainstem) and any remaining smaller volume tumor is then treated subsequently with radiosurgery / SRT / FSR / Micro (MLC) Radiosurgery.
Conclusions:
With modern diagnostic methods acoustic neuromas and other cranial schwannomas can be diagnosed earlier when they are smaller and have lesser symptoms and lesser brain and nerve damage. Modern treatment methods including no surgery methods as described above have improved treatment success and allowing more people to have a better quality and length of life.
