Craniopharyngioma
Craniopharyngiomas are benign brain tumors (not a cancer). They can affect children and adults.
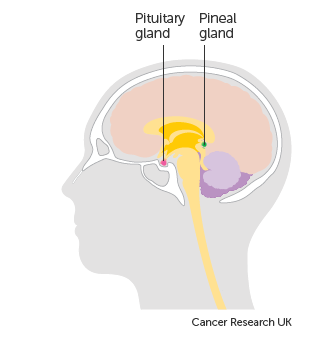
Craniopharyngiomas usually grow near the base of the brain, just above the pituitary gland. The pituitary gland makes hormones that control important body functions.
Craniopharyngiomas do not usually spread. Because they grow close to the pituitary gland, they can cause changes in the way that it works. Symptoms of craniopharyngiomas include:
- changes in hormone levels. In adults this might cause difficulty getting an erection and irregular periods. It can also cause growth problems in children and diabetes
- loss of eyesight
- headaches
- a build up of pressure in and around the brain, which can cause feeling or being sick
Symptoms can develop suddenly, which means that you feel unwell quickly or they can develop more slowly.
How common it is
Craniopharyngiomas are not common tumors. In children, between 6 and 13 out of every 100 brain tumors (6 to 13%) are craniopharyngiomas. And in adults, between 1 and 3 out of every 100 brain tumors (1 to 3%) are craniopharyngiomas.
What tests will I have?
To find out what is causing your symptoms our Neurosurgeon will arrange for you to have some tests. The tests you might have include:
- blood tests to look at the levels of hormones
- MRI brain scan or CT brain scan
- eye examinations including Fundal examination of the optic nerve
- a biopsy
As well as finding out whether you have a tumor, the tests check the size of the tumor and its location.
Treatment
According to Dr Prem Pillay a Singapore Neurosurgeon, (trained at the Cleveland Clinic -USA,MD Anderson Cancer Center-USA and the Hospital for Sick Children, Toronto) an expert on Craniopharyngiomas, microsurgery either through a craniotomy or through Endoscopic surgery through the nose to attempt complete tumor removal is usually recommended. In patients where the tumor cannot be completely removed safely or where patients decline surgery Radiotherapy especially more advanced methods like Stereotactic Radiotherapy using Micro MLC technology or Radiosurgery can be used. Proton Therapy is another advanced technology that can be used. Hormone replacement therapy may be needed if there are changes in the levels of hormones.
Surgery Specifics
A brain specialist surgeon (neurosurgeon) removes all the tumor or just a part depending on where the tumor is.
Some tumors are close to important parts of the brain such as the optic nerve and the hypothalamus. These tumors cannot usually be completely removed.
The side effects you might have after the operation include:
- changes in the hormone levels
- high blood sugar levels (diabetes)
- changes in vision
- weight gain
- behaviour changes
Radiotherapy
If there is residual tumor you may have Stereotactic radiotherapy after surgery. This is to try to stop the tumor from coming back. You might also have radiotherapy if the tumor comes back. For small tumors, you might have stereotactic radiotherapy or radiosurgery. Both treatments target high doses of radiotherapy to the tumor. Some people may also have a type of radiotherapy called proton beam therapy. It uses high energy or low energy proton beams to the tumor.
Hormone replacement
Many people with a craniopharyngioma have changes in their hormone levels. This is due to either the tumor itself or as a side effect of treatment. You might need to take hormone replacement therapy to help with this. The type of hormone you take depends on your individual needs.
Follow up
You have regular appointments with your doctor after treatment finishes. Your doctor examines you at each appointment. They ask how you are feeling, whether you have had any symptoms or side effects and if you are worried about anything. You might also have MRI scans on some visits.
How often you have check ups depends on your individual situation. Most people have a check up every 6 to 12 months, for up to 5 years.
Coping with craniopharyngioma
Coping with a diagnosis of a brain tumor can be difficult, both practically and emotionally. It can be especially difficult when you have a uncommon tumor. Being well informed about the type of tumor you have, and its treatment can make it easier to cope.
Craniopharyngiomas are rare malformational tumours of low histological malignancy arising along the craniopharyngeal duct. The two histological subtypes, adamantinomatous craniopharyngioma (ACP) and papillary craniopharyngioma (PCP), differ in genesis and age distribution. ACPs are diagnosed with a bimodal peak of incidence (5–15 years and 45–60 years), whereas PCPs are restricted to adults mainly in the fifth and sixth decades of life. ACPs are driven by somatic mutations in CTNNB1 (encoding β-catenin) that affect β-catenin stability and are predominantly cystic in appearance. PCPs frequently harbour somatic BRAFV600E mutations and are typically solid tumours. Clinical manifestations due to increased intracranial pressure, visual impairment and endocrine deficiencies should prompt imaging investigations, preferentially MRI. Treatment comprises neurosurgery and radiotherapy; intracystic chemotherapy is used in monocystic ACP. Although long-term survival is high, quality of life and neuropsychological function are frequently impaired due to the close anatomical proximity to the optic chiasm, hypothalamus and pituitary gland. Indeed, hypothalamic involvement and treatment-related hypothalamic lesions frequently result in hypothalamic obesity, physical fatigue and psychosocial deficits. Given the rarity of these tumours, efforts to optimize infrastructure and international collaboration should be research priorities. Dr Prem Pillay a Neurosurgeon who specializes in the treatment of these brain tumors agrees and notes that advances in Neurosurgery and Neurosciences including Molecular biology and Genetics will help achieve better results for those with this disease.
References
Singapore Brain Spine Nerves Center Protocols and information
Cancer UK information
