PERIPHERAL NERVE TUMORS
DR PREM PILLAY,
SENIOR CONSULTANT NEUROSURGEON
PERIPHERAL NERVE TUMORS EXPERT
SINGAPORE
Overview and Classification


Peripheral nerve tumors are a heterogeneous group of neoplasms that arise from or affect nerves outside the brain and spinal cord [4][8]. According to the 2021 WHO classification of the Central Nervous System (CNS), peripheral nerve sheath tumors (PNSTs) comprise a set of unique entities each with specific clinical, anatomical, histological, and molecular features [1]. Broadly, PNSTs can be subdivided into benign and malignant forms, often reflecting differences in their behavior, prognosis, and recommended treatments.
Benign Peripheral Nerve Sheath Tumors
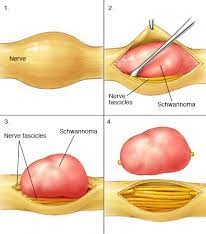
- Schwannoma
Schwannomas originate from Schwann cells, which form the myelin sheath of peripheral nerves [1][8]. Most schwannomas are benign and can appear anywhere along peripheral nerves. Variants include plexiform schwannoma, which can arise in superficial or deep sites and may be challenging to distinguish from more aggressive lesions if they show atypical features [1][8]. Multiple schwannomas may be associated with NF1 (Neurofibromatosis). Patients with a peripheral nerve schwannoma may need to have screening of other nerves with MRI of the whole spine and Brain with gadolinium contrast to rule out multiple nerve tumors at other locations.
- Neurofibroma
Neurofibromas also arise from Schwann cells, typically featuring other non-neoplastic cellular components (e.g., fibroblasts, perineurial cells) [8]. A distinct subtype is the **plexiform neurofibroma**, often linked to neurofibromatosis type 1 (NF1). Plexiform neurofibromas can transform into malignant peripheral nerve sheath tumors (MPNSTs) and therefore warrant close monitoring [1][8].
- Perineurioma and Hybrid Nerve Sheath Tumors
Perineuriomas exhibit differentiation toward perineurial cells, while hybrid nerve sheath tumors can show areas of both schwannoma and neurofibroma (or other) histology [1][8]. These tumors are relatively rare but are increasingly recognized due to improved molecular diagnostics.
Malignant Peripheral Nerve Sheath Tumors (MPNST)
MPNSTs are aggressive soft-tissue sarcomas accounting for about 10% or slightly more of all peripheral nerve sheath tumors [4][5]. They may arise sporadically or in association with NF1 or prior radiation therapy [1][5]. MPNSTs often present with a high risk of local recurrence and metastasis, with the prognosis highly dependent on complete surgical resection and the tumor’s stage at diagnosis [5][10].
Clinical Presentation and Diagnosis
Peripheral nerve tumors can present with:
-Localized or diffuse swelling along the nerve path
– Neurological deficits such as numbness, pain, tingling, or muscle weakness in an arm or leg
– Positive Tinel or Hoffman-Tinel sign , indicative of nerve irritation [4]
Imaging studies are central in delineating the location and extent of the tumor:
- Magnetic Resonance Imaging (MRI)
Considered the gold standard for visualizing peripheral nerve tumors, MRI provides high-resolution images that can define the relationship between the tumor and adjacent structures [1][2][7]. Certain MRI sequences (such as diffusion-weighted imaging) are investigated for differentiating benign from malignant lesions [5].
- Computed Tomography (CT)
Can be used to further assess bony involvement or complex anatomical regions, supplementing MRI findings [2].
- Positron Emission Tomography (PET)
Useful in more complex cases, particularly for detecting malignant transformation and metastatic spread, although its use is often guided by specific clinical scenarios [1][8].
- Electromyogram (EMG)
EMG and nerve conduction studies can help assess the functional impact on the peripheral nerve [2].
- Biopsy
A core or excisional biopsy is typically performed to confirm histopathology, determine tumor grade, and guide treatment decisions [2][7][8].
Treatment Approaches
Watchful Waiting
In asymptomatic, slowly growing, small benign peripheral nerve tumors (usually a few mm in size) a watch-and-wait approach (also called “monitoring”) may be considered if they do not threaten function [3][7]. Periodic MRI or other imaging helps track any changes in size or symptoms, and treatment can be initiated if the tumor grows or becomes symptomatic.
Surgery
Micro-surgical resection remains the mainstay of therapy for most peripheral nerve tumors, both benign and malignant [3][4][7][10]. In benign lesions such as schwannomas or neurofibromas, careful microsurgical removal can often be curative. For MPNSTs, wide surgical margins are crucial for potential cure [10] with nerve grafting where required. However, surgical planning must balance tumor removal with functional nerve preservation.
Radiotherapy
– Adjuvant Radiotherapy: Often recommended for malignant peripheral nerve sheath tumors with larger lesion sizes or aggressive histological features [10]. It can also be used if resection margins are close to the spinal cord or large nerve plexus or if a tumor is not fully resectable.
– Stereotactic Radiosurgery: Precisely delivers radiation to limit damage to nearby structures. It is used for tumors along cranial nerves or near to the Spinal Cord or if a tumor is not fully resectable without causing functional issues[2][3][7].
Chemotherapy
Chemotherapy sensitivity varies among peripheral nerve tumors. **MPNSTs**, unfortunately, do not respond robustly to conventional chemotherapy, though anthracycline-based regimens may be tried in inoperable or metastatic settings [1][9]. In NF1-associated tumors, chemotherapy or newer targeted agents may be considered, particularly in children with symptomatic plexiform neurofibromas [1][5].
Targeted and Molecular Therapies
Research into molecular pathways involved in PNSTs, especially MPNSTs, has propelled the exploration of targeted agents:
- MEK Inhibitors
Selumetinib is approved for children ≥2 years with NF1-related plexiform neurofibromas that are inoperable or symptomatic, demonstrating tumor shrinkage in some cases [1][5]. Other MEK1/2 inhibitors are under clinical investigation.
- mTOR Inhibitors
Combinations of MEK and mTOR inhibitors are being tested to broaden therapy options and potentially reduce tumor growth [1][5].
- Immunotherapy and Other Targeted Pathways
Emerging evidence suggests that immunomodulatory approaches or other molecularly guided treatments may benefit a subset of aggressive MPNSTs, though these remain experimental [5]. Clinical trials continue to assess efficacy.
Latest Innovations and Future Directions
– Molecular Diagnostics : Advanced genetic profiling (e.g., next-generation sequencing) helps distinguish between atypical neurofibromas and early malignant transformation [8]. Improved understanding of tumor biology is critical for identifying actionable targets.
– Refined Imaging Techniques : Sophisticated MRI protocols, including diffusion-weighted imaging and contrast-enhanced sequences, improve the detection and characterization of subtle nerve lesions and can aid in surgical planning [1][5].
– Minimally Invasive Surgical Techniques : Refined microsurgical instruments and computer-assisted navigation allow safer resections with enhanced functional preservation [7].
– Combination Therapies : Ongoing clinical trials are exploring the combined use of targeted drugs (MEK, mTOR inhibitors) and traditional treatments (radiotherapy, chemotherapy) to improve outcomes in MPNSTs [1][5].
Conclusion
Peripheral nerve tumors, encompassing benign entities such as schwannomas and neurofibromas and malignant variants like MPNSTs, represent a diverse group requiring careful workup and multidisciplinary treatment. Accurate diagnosis via imaging and biopsy, alongside precision surgical techniques, can often lead to remission in benign lesions and offer the best chance for disease control in malignant ones. Meanwhile, current innovations in targeted therapy, molecular diagnostics, and radiation approaches hold promise for improving outcomes in these rare yet complex tumors [1][5][7][8][10]. Dr Prem Pillay explains that ongoing research and collaboration among neurosurgeons, neuroscientists, and patient advocacy groups are essential to further refine therapies, minimize side effects, and enhance quality of life for individuals with peripheral nerve tumors.
With many years of experience in treating peripheral nerve tumors and access to the latest technological advancements, Dr Prem Pillay endevours to offer patients the highest standard of care. From accurate diagnosis to tailored treatment plans, our approach aims for the best possible outcomes for individuals affected by this challenging condition.
If you or a loved one has been diagnosed with a peripheral Nerve Tumor , we welcome you to seek consultation with our specialist and his team. Together, we can develop comprehensive evidence based and personalized treatment strategy that addresses your unique needs and provides the best chance for a positive outcome.
References:
[1] https://pmc.ncbi.nlm.nih.gov/articles/PMC10093509/
[2] https://www.mayoclinic.org/diseases-conditions/peripheral-nerve-tumors/diagnosis-treatment/drc-20355075
[3] https://www.uofmhealthsparrow.org/departments-conditions/conditions/peripheral-nerve-tumors
[4] https://pmc.ncbi.nlm.nih.gov/articles/PMC11031624/
[5] https://pmc.ncbi.nlm.nih.gov/articles/PMC9954030/
[6] https://www.ohsu.edu/brain-institute/nerve-tumors
[7] https://neurosurgery.weillcornell.org/condition/peripheral-nerve-sheath-tumors/treatment-peripheral-nerve-sheath-tumors
[8] https://pmc.ncbi.nlm.nih.gov/articles/PMC3629555/
[9] https://www.cancerresearchuk.org/about-cancer/soft-tissue-sarcoma/types/malignant-schwannoma
[10] https://pubmed.ncbi.nlm.nih.gov/25777573/
