Chiari malformations
Dr Prem Pillay,
Senior Consultant Adult and Pediatric Neurosurgeon:
Spine Specialist and Expert in Chiari Malformations
What are Chiari malformations?

Chiari malformations (CM) are structural defects in the base of the skull and cerebellum, the part of the brain that controls balance. Normally the cerebellum and parts of the brain stem sit above an opening in the skull that allows the spinal cord to pass through it (called the foramen magnum). When part of the cerebellum extends below the foramen magnum and into the upper spinal canal, it is called a Chiari malformation (CM).
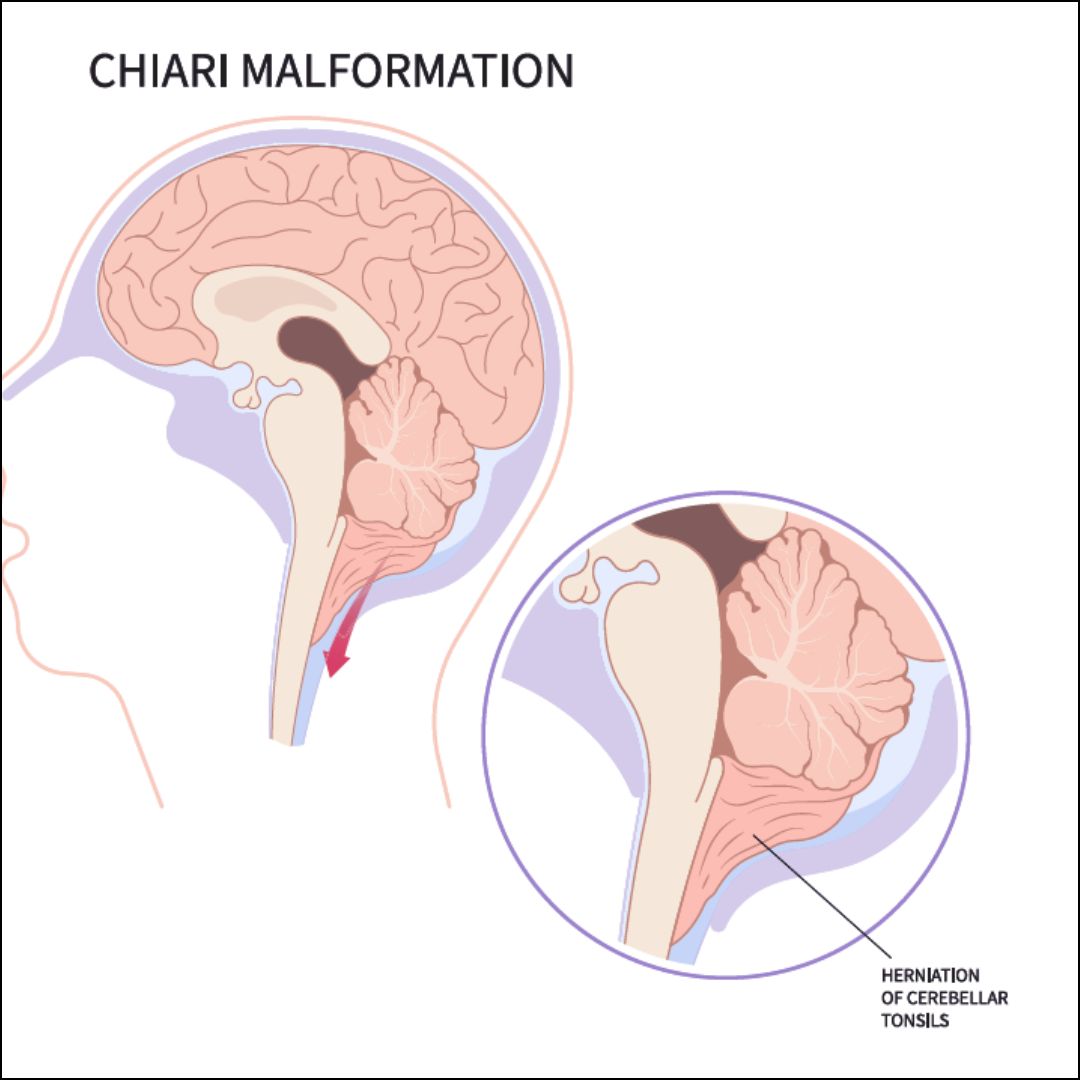
Chiari malformations may develop when part of the skull is smaller than normal or misshapen, which forces the cerebellum to be pushed down into the foramen magnum and spinal canal. This causes pressure on the cerebellum and brain stem that may affect functions controlled by these areas and block the flow of cerebrospinal fluid (CSF)—the clear liquid that surrounds and cushions the brain and spinal cord. The CSF also circulates nutrients and chemicals filtered from the blood and removes waste products from the brain.
What causes these malformations?
CM has several different causes. It is caused by structural defects in the brain and spinal cord that occur during development or in later life from injury, tumor, disease or infection. The chiari that occurs in early life can be the result of genetic mutations or a maternal diet that lacked certain vitamins or nutrients. This is called primary Chiari malformation. It can also be caused later in life if spinal fluid is drained excessively from the lumbar or thoracic areas of the spine either due to traumatic injury, disease, or infection. This is called acquired or secondary Chiari malformation.
What are the symptoms of a Chiari malformation?
According to Dr Prem Pillay , an Expert in the field of Neurosurgery and Chiari Malformations , Headache is the hallmark sign of Chiari malformation, which can be aggravated by sudden coughing, sneezing, or straining. Symptoms may vary among individuals and may include one or more of the following:
- Headache
- Neck Pain
- hearing or balance problems
- muscle weakness or numbness
- numbness in the face, arms or legs
- a burning sensation in the fingers, toes or lips
- dizziness
- difficulty swallowing or speaking
- vision changes like double vision and blurred vision
- vomiting
- ringing or buzzing in the ears (tinnitus) and hearing loss
- curvature of the spine (scoliosis)
- insomnia
- depression
- sleep apnea
- chronic fatigue
- problems with hand coordination and fine motor skills.
People with Chiari Malformation may have a combination of some or all of the above symptoms. Some individuals with CM may not show any symptoms. Symptoms may change for some individuals, depending on the compression of the tissue and nerves and on the buildup of CSF pressure.
Infants with a Chiari malformation may have difficulty swallowing, irritability when being fed, excessive drooling, a weak cry, gagging or vomiting, arm weakness, a stiff neck, breathing problems, developmental delays, and an inability to gain weight.
How are CMs classified?
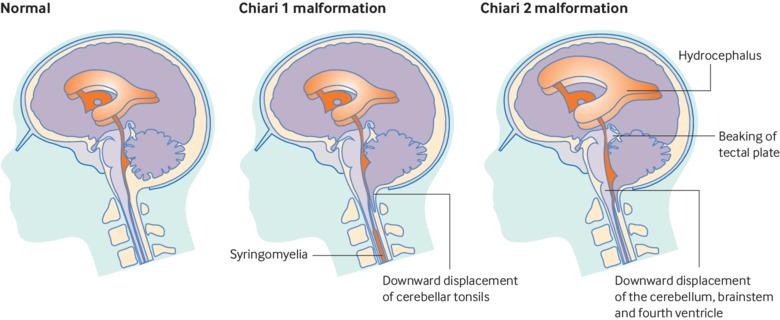
Chiari malformations are classified by the severity of the disorder and the parts of the brain that protrude into the spinal canal.
Chiari malformation Type I
Type 1 happens when the lower part of the cerebellum (called the cerebellar tonsils) extends into the foramen magnum. Normally, only the spinal cord passes through this opening. Type 1—which may not cause symptoms—is the most common form of CM. It is usually first noticed in adolescence or adulthood, often by accident during an examination for another condition. Adolescents and adults who have CM but no symptoms initially may develop signs of the disorder later in life said Dr Prem Pillay.
Chiari malformation Type II
Individuals with Type II have symptoms that are generally more severe than in Type 1 and usually appear during childhood. This disorder can cause life-threatening complications during infancy or early childhood, and treating it requires surgery.
In Type II, also called classic CM, both the cerebellum and brain stem tissue protrude into the foramen magnum. Also the nerve tissue that connects the two halves of the cerebellum may be missing or only partially formed. Type II is usually accompanied by a myelomeningocele—a form of spina bifida that occurs when the spinal canal and backbone do not close before birth. (Spina bifida is a disorder characterized by the incomplete development of the brain, spinal cord, and/or their protective covering.) A myelomeningocele usually results in partial or complete paralysis of the area below the spinal opening. The term Arnold-Chiari malformation (named after two pioneering researchers) is specific to Type II malformations.
Chiari malformation Type III
Type III is very rare and the most serious form of Chiari malformation. In Type III, some of the cerebellum and the brain stem stick out, or herniate, through an abnormal opening in the back of the skull. This can also include the membranes surrounding the brain or spinal cord.
The symptoms of Type III appear in infancy and can cause debilitating and life-threatening complications. Babies with Type III can have many of the same symptoms as those with Type II but can also have additional severe neurological defects such as mental and physical delays, and seizures.
Chiari malformation Type IV
Type IV involves an incomplete or underdeveloped cerebellum (a condition known as cerebellar hypoplasia). In this rare form of CM, the cerebellum is located in its normal position but parts of it are missing, and portions of the skull and spinal cord may be visible.
What other conditions are associated with Chiari malformations?
Hydrocephalus is an excessive buildup of CSF in the brain. A CM can block the normal flow of this fluid and cause pressure within the head that can result in mental defects and/or an enlarged or misshapen skull. Severe hydrocephalus, if left untreated, can be fatal. The disorder can occur with any type of Chiari malformation, but is most commonly associated with Type II. Spina bifida is the incomplete closing of the backbone and membranes around the spinal cord. In babies with spina bifida, the bones around the spinal cord do not form properly, causing defects in the lower spine. While most children with this birth defect have such a mild form that they have no neurological problems, individuals with Type II Chiari malformation usually have myelomeningocele, and a baby’s spinal cord remains open in one area of the back and lower spine. The membranes and spinal cord protrude through the opening in the spine, creating a sac on the baby’s back. This can cause a number of neurological impairments such as muscle weakness, paralysis, and scoliosis.
Syringomyelia is a disorder in which a CSF-filled tubular cyst, or syrinx, forms within the spinal cord’s central canal. The growing syrinx destroys the center of the spinal cord, resulting in pain, weakness, and stiffness in the back, shoulders, arms, or legs. Other symptoms may include a loss of the ability to feel extremes of hot or cold, especially in the hands. Some individuals also have severe arm and neck pain.
Tethered cord syndrome occurs when a child’s spinal cord abnormally attaches to the tissues around the bottom of the spine. This means the spinal cord cannot move freely within the spinal canal. As a child grows, the disorder worsens, and can result in permanent damage to the nerves that control the muscles in the lower body and legs. Children who have a myelomeningocele have an increased risk of developing a tethered cord later in life and therefore need follow up said Dr Prem Pillay.
Spinal curvature is common among individuals with syringomyelia or CM Type I. The spine either may bend to the left or right (scoliosis) or may bend forward (kyphosis).
How common are Chiari malformations?
In the past, it was estimated that the condition occurs in about one in every 1,000 people. However, says Dr Prem , the increased use of diagnostic imaging for the Brain and upper Spine such as MRI (Magnetic Resonance Imaging ) has shown that Chiari malformation may be much more common. Complicating this estimation is the fact that some children who are born with this condition may never develop symptoms or show symptoms only in adolescence or adulthood. Chiari malformations occur more often in women than in men and Type II malformations are more prevalent in certain groups, including people of Celtic descent.
How are Chiari malformations diagnosed?
Currently, no test is available to determine if a baby will be born with a Chiari malformation. Since Chiari malformations are associated with certain birth defects like spina bifida, children born with those defects are often tested for malformations. However, some malformations can be seen on ultrasound images before birth.
Many people with Chiari malformations have no symptoms and their malformations are discovered only during the course of diagnosis or treatment for another disorder. According to Dr Prem a Neurological examination includes a physical exam and checking the person’s memory, cognition, balance (functions controlled by the cerebellum), touch, reflexes, sensation, and motor skills (functions controlled by the spinal cord). The Neurosurgeon may also order one or more of the following diagnostic tests:
- Magnetic resonance imaging (MRI) is the imaging procedure most often used to diagnose a Chiari malformation. It uses a powerful magnetic field to painlessly produce either a detailed three-dimensional picture or a two-dimensional “slice” of body structures, including tissues, organs, bones, and nerves.
- X-rays use electromagnetic energy to produce images of bones and certain tissues on film. An X-ray of the head and neck cannot reveal a CM but can identify bone abnormalities that are often associated with the disorder.
- Computed tomography (CT) uses X-rays and a computer to produce two-dimensional pictures of bone and blood vessels. CT can identify hydrocephalus and bone abnormalities associated with Chiari malformation.
How are Chiari malformations treated?
Some CMs do not show symptoms and do not interfere with a person’s activities of daily living. In these cases, said Dr Prem, we may only recommend regular monitoring with MRI. When individuals experience pain or headaches, we may prescribe medications to help ease symptoms. However some people continue to have headaches and may also develop pain, numbness and weakness in the hands, arms or legs related to progressive damage to the central nervous system and or spinal cord. These patients will need to consider surgery. Patients with large syringomyelia or progressing syrinxes will also need to consider surgery. Surgery for the Chiari Malformation alone is often enough to treat the syringomyelia as well.
Surgery / Microsurgery
In many cases, surgery is the only treatment available to ease symptoms or halt the progression of damage to the central nervous system. Surgery can improve or stabilize symptoms in most individuals.
The most common surgery to treat Chiari malformation is a Microsurgery: posterior fossa decompression. It creates more space for the cerebellum and relieves pressure on the spinal cord. The surgery involves making an incision at the back of the head and removing a small portion of the bone at the bottom of the skull (craniectomy) using fine Micro drills. In some cases the arched, bony roof of the spinal canal, called the lamina, may also be removed (spinal laminectomy). The surgery should help restore the normal flow of CSF, and be enough to relieve symptoms and prevent neurological deterioration in most people.
Next, the surgeon may make an incision in the dura, the protective covering of the brain and spinal cord. If the brain and spinal cord area is still crowded, the surgeon may use a procedure called Bipolar cautery or a Laser to remove/reduce the cerebellar tonsils, allowing for more free space. These tonsils do not have a recognized function and can be removed without causing any known neurological problems.
The final step is to sew a dura patch to expand the space around the tonsils, similar to letting out the waistband on a pair of pants. This patch can be made of artificial material or tissue harvested from another part of an individual’s body.
Infants and children with myelomeningocele may require surgery to reposition the spinal cord and close the opening in the back. Findings from the National Institutes of Health (NIH) show that this surgery is most effective when it is done prenatally (while the baby is still in the womb) instead of after birth. The prenatal surgery reduces the occurrence of hydrocephalus and restores the cerebellum and brain stem to a more normal alignment.
Hydrocephalus may be treated with a shunt (tube) system that drains excess fluid and relieves pressure inside the head. A sturdy tube, surgically inserted into the head, is connected to a flexible tube placed under the skin. These tubes drain the excess fluid into either the chest cavity or the abdomen so it can be absorbed by the body.
An alternative surgical treatment in some individuals with hydrocephalus is third ventriculostomy, a procedure that improves the flow of CSF out of the brain. A Brain Endoscope is used to enter the Lateral Ventricle and a small hole is made at the bottom of the third ventricle (brain cavity) and the CSF is diverted there to relieve pressure. Similarly, in cases where surgery was not effective enough, doctors may open the spinal cord and insert a shunt (Syringo Subarachnoid shunt or syringo-peritoneal shunt )to drain a syringomyelia or hydromyelia (increased fluid in the central canal of the spinal cord).
What research is being done?
Genetics
The NIH and other research entities are researching the genetic factors that increase the risk of developing Chiari malformation and related brain disorders. Recent studies have identified gene mutations in the PI3K-AKT signaling pathway that cause brain overgrowth that may accompany hydrocephalus, CM, and other brain disorders. To better understand the genetic factors responsible for Chiari I malformation, NINDS scientists are looking for other gene mutations that could act through PI3K-AKT signaling and other pathways. These studies could lead to new diagnostic tests and better treatments options for Chiari malformations and other developmental brain disorders.
Brain mechanisms
Certain signals at the midbrain-hindbrain (MHB) boundary tell the brain to properly develop the cerebellum and other parts of the brain. However, how these brain regions are initiated, formed, and maintained is not well understood. Neuroscientists are studying zebrafish embryos in order to gain a better understanding of how the MHB forms. This will provide valuable insights into human brain development, particularly the cerebellum. Other investigators are studying the expression of different growth factors on the development of the brain, skull, spine, and spinal cord. Interference with normal gene function through gene mutation or environmental factors may influence the development of CM.
Conclusions
There are many people who have Chiari Malformation but are unaware about it until it becomes more serious. Early symptoms including headaches and neck pain are often dismissed as being not serious. Chiari Malformations can now be better diagnosed and treated. The use of more advanced MRI technology, Computer Image-Guided Microsurgery with Microinstruments , together with Electrical/Electronic monitoring of the central nervous system during surgery , and computer aided Neuronavigation has made better and safer treatment possible states Dr Prem Pillay.
With many years of experience in treating Chiari Malformations and Syringomyelia and access to the latest technological advancements, Dr Prem Pillay endeavours to offer patients the highest standard of care. From accurate diagnosis to tailored treatment plans, our approach aims for the best possible outcomes for individuals affected by this challenging condition.
If you or a loved one has been diagnosed with a Chiari Malformation problem, we welcome you to seek consultation with our specialized team. Together, we can develop a comprehensive evidence based and personalized treatment strategy that addresses your unique needs and provides the best chance for a positive outcome.
References
National Institute of Health – USA: Information at www.ninds.nih.gov
The Cleveland Clinic Foundation: Information at www.my.clevelandclinic.org
Singapore Brain Spine Nerves Center: Protocols and Information at www.singaporebrain.org
